Tests to assess liver function :
The liver function tests (LFT) are the biochemical investigations to assess the capacity of the liver to carry out any of the functions it performs. LFT will help to detect the abnormalities and the extent of liver damage.
Two important facts should be borne in mind while carrying out LFT.
• Liver is a large-size factory of safety. Therefore, it can perform many of its functions almost normally, despite the damage.
• Selection of the right test is important in LFT. This is due to the fact that since liver participates in several functions, the function that is measured in LFT may not be the one that is adversely affected. The major liver function tests may be classified based on :
a. Excretory function - Measurement of bile pigments, bile salts, bromosulphthalein.
b. Serum enzymes derived from liver - Determination of transaminases, alkaline phosphatase, 5'-nucleotidase, y-glutamyl-transpeptidase.
c. Metabolic capacity - Galactose tolerance, antipyrine clearance.
d. Synthetic functions - Prothrombin time, serum albumin.
e. Detoxification - Hippuric acid synthesis.
The choice of biochemical tests to measure liver functions mostly depends on the purpose of the investigation.
The clinical history of the subject is often a guiding factor in this regard.
A single test in isolation may have a little diagnostic value.
Frequently, a combination of laboratory investigations are employed in LFT.
These include serum bilirubin (conjugated and unconjugated), alanine transaminase, aspartate transaminase, alkaline phosphatase, y-glutamyl transpeptidase and proteins (albumin, globulins). The most commonly used tests include the estimation of levels of serum enzymes.
PROBLEM STATEMENT
How can serum biochemical analysis detect and differentiate patterns of liver injury? What is the laboratory workflow for precise, reliable transaminase measurement? How can these results be interpreted to distinguish between acute, chronic, or non-hepatic causes of elevated enzyme activity?
Transaminases in assessing liver function :
Liver cells contain several enzymes which may be released into the circulation in liver damage. Measurement of selected enzymes in serum is often used to assess the liver function.
It must, however, be noted that there is no single enzyme that is absolutely specific to liver alone. Despite this fact, serum enzymes provide valuable information for LFT.
The activities of two enzymes -
serum glutamate pyruvate transaminase (SGPT; now called alanine transaminase - ALT)
serum glutamate oxaloacetate transaminase (SGOT; now called aspartate transaminase - AST) -
It is widely used to assess the liver function by the Reitman and Frankel method.
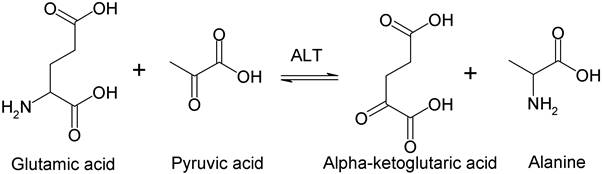
Transamination is the term given to the process in which an amino group is transferred from an a amino acid to an α-keto acid.
As a result, different a amino acids and α-keto acids are formed.
All naturally occurring a amino acids can take part in such reactions, each with their specific enzymes.
The enzymes that carry out transamination are called transaminases and their function is to retain amino groups during amino-acid breakdown by transferring the amino group from the amino acid to a keto acid.
They are found in many tissues including heart, liver, kidney, and muscle. Two such important enzymes are glutamate-oxaloacetate transaminase and glutamate-pyruvate transaminase.
SGPT - ALT
SGOT - AST

ALT is a cytoplasmic enzyme while AST is found in both cytoplasm and mitochondria.
The activity of these enzymes is low in normal serum.
Serum ALT and AST are increased in liver damage.
However, alanine trans-aminase is more sensitive and reliable for the assessment of LFT.
The normal AST/ALT ratio is around 0.8.
This ratio is increased (>2) in myocardial infarction, alcoholic hepatitis, and cirrhosis.
AST/ALT ratio is decreased (i.e. ALT higher) in acute hepatocellular damage and cholestasis.
Principle:
The estimation of SGOT and SGPT is done by the Rietmen and Frankel's method.
In the method, the activity of transaminases (aminotransferases) is determined by measuring the colour of the hydrazone (brown) which is formed by the reaction between 2,4-dinitrophenyl hydrazine (DNPH) and the ketoacid, a products of transaminase reaction; and is highly coloured in alkaline medium.
DNPH reacts with all oxoacids. These include oxoglutarate and oxaloacetate, as well as pyruvate, which are on the two sides of the above equations.
DNPH gives more colour with oxaloacetate and pyruvate than with oxoglutarate, thus making the method feasible with an acceptable limit of error.
In both estimations - ALT and AST, the substrates are suboptimal, to reduce the background colour given by the alpha-ketoglutarate (or oxoglutarate) in the reaction with DNPH.

Though not as accurate as spectrophotometric method (UV) which measures decrease in the absorbance at 340 nm as NADH as it is consumed in the reaction (NAD has no absorbance), the colorimetric method is easily adaptable and is much faster to perform than the spectrophotometric method.
REQUIREMENTS
Chemicals/Reagents:
-
M/15 Phosphate buffer, pH 7.4
-
SGOT substrate: 2.66 g aspartic acid, 30 mg α-ketoglutarate, 20.5 mL 1N NaOH; bring to 100 mL in buffer, pH 7.4
-
SGPT substrate: 1.78 g alanine, 30 mg α-ketoglutarate, 1.25 mL 0.4N NaOH; bring to 100 mL in buffer, pH 7.4
-
DNPH reagent: 200 mg DNPH, 85 mL conc. HCl, make up to 1000 mL distilled water
-
0.4N NaOH
-
Sodium pyruvate standard (22 mg/dL)
Apparatus/Glassware:
-
Water bath/incubator at 37°C
-
Colorimeter/spectrophotometer (530 nm)
-
Graduated test tubes and pipettes
-
Refrigerator (for substrate storage; add chloroform preservative if required)
-
Stopwatch or timer
PROTOCOL
A. Preparation of Standard Calibration Curve
-
Prepare tubes with varying volumes of SGOT or SGPT substrate and sodium pyruvate standard as follows:
| Tube | Substrate (ml) | Pyruvate Std. (ml) | dH₂O (ml) | DNPH (ml) | NaOH (ml) | Karmen Units |
|---|---|---|---|---|---|---|
| 1 | 0.45 | 0.05 | 0.10 | 0.5 | 5 | 27 |
| 2 | 0.40 | 0.10 | 0.10 | 0.5 | 5 | 61 |
| 3 | 0.35 | 0.15 | 0.10 | 0.5 | 5 | 114 |
| 4 | 0.30 | 0.20 | 0.10 | 0.5 | 5 | 190 |
| Blank | 0.50 | — | 0.10 | 0.5 | 5 | 0 |
-
Mix all solutions, incubate at room temperature for 20 minutes.
-
Add 5 mL of 0.4N NaOH, mix thoroughly, incubate for 10 minutes.
-
Measure the absorbance at 530 nm for each tube.
-
Plot calibration curve: Karmen units (X-axis) vs absorbance (Y-axis).
B. Assay of Serum Test Sample
-
Pipette 0.5 ml substrate (SGOT or SGPT, prewarmed at 37°C) into a test tube.
-
Add 0.1 ml serum sample.
-
Incubate at 37°C for:
-
SGOT: 60 minutes
-
SGPT: 30 minutes
-
-
Add 0.5 ml DNPH, mix, leave at room temperature for 20 minutes.
-
Add 5 ml 0.4N NaOH, mix, leave at room temperature for another 10 minutes.
-
Measure test tube absorbance at 530 nm.
For liver function tests : SGPT and SGOT :
1. Preparation of standard graph for GOT / GPT assay :
|
|
1 |
2 |
3 |
4 |
Blank |
|
GOT / GPT substrate (ml) |
0.45 |
0.4 |
0.35 |
0.3 |
0.5 |
|
Std. Sodium pyruvate (ml) |
0.05 |
0.1 |
0.15 |
0.2 |
- |
|
Distilled water (ml) |
0.1 |
0.1 |
0.1 |
0.1 |
0.1 |
|
DNPH reagent (ml) |
0.5 |
0.5 |
0.5 |
0.5 |
0.5 |
|
Mix thoroughly, keep at room temperature for 20 minutes. |
|||||
|
0.4N NaOH. (ml) |
5 |
5 |
5 |
5 |
5 |
|
Karmen units (GOT) |
27 |
61 |
114 |
190 |
0 |
|
Karmen units (GPT) |
28 |
57 |
97 |
150 |
0 |
|
Mix and keep at room temperature for 10 minutes. Read absorbance at 530 nm. |
|||||
|
A 530 GOT |
|
|
|
|
|
|
A 530 GPT |
|
|
|
|
|
Draw a curve of Karmen units on X axis versus absorbance on Y axis
2. Treatment of test sample :
• To 0.5 ml of GOT / GPT substrate prewarmed to 37°C, add 0.1 ml of serum and incubate at 37°C for 60 minutes for GOT / 30 minutes for GPT.
• Add 0.5 ml of DNPH. Mix thoroughly, keep at room temperature for 20 minutes.
• Add 5 ml of 0.4N NaOH. Mix and keep at room temperature for 10 minutes.
• Read absorbance at 530 nm.
ormal value :
The adult reference range for both AST and ALT is roughly 10-40 U/L i.e. 20.83 - 83.33 Karmen Units when measured at 37°C.
Although men have slightly higher values than women do, most laboratories use a single range for both genders.
Note :
• Karmen unit/ ml is equivalent to 0.48 U/L.
• The GOT / GPT substrate can be preserved in refrigerator by adding 1 ml of chloroform. Discard the substrate solution on appearance of turbidity.
CALCULATION & GRAPH
Karmen unit:
A Karmen unit is defined as the amount of enzyme required to produce enough pyruvic acid in 1 mL of serum in a reaction volume of 3 mL, at 25°C, that causes a decrease in NADH absorbance by 0.001 per minute in a spectrophotometric assay. In the colorimetric DNPH method used by Reitman & Frankel, this relates to the amount of pyruvate formed that reacts to give a measurable color.
Purpose:
Karmen units quantify the enzyme activity in the given sample, expressing how much substrate (e.g., pyruvate) is produced per unit time by the transaminase enzyme.
The graph used in the Reitman & Frankel colorimetric test is a calibration curve that helps turn color readings from the experiment into actual enzyme activity values.
What does the graph look like?
-
On the X-axis (horizontal) are numbers called Karmen units, which are values that match known amounts of the product (pyruvate or oxaloacetate).
-
On the Y-axis (vertical) are the absorbance values, measured with a colorimeter at 530 nm, telling you how dark the color in each tube is after the reaction.
Why do we make this graph?
When you do the experiment, you'll get a color in each tube (from the hydrazone reaction), and you'll measure how strong that color is using the colorimeter. But you need to know what that color strength means in terms of actual enzyme activity. The calibration graph shows what absorbance (color intensity) is expected for each known Karmen unit.
How is the graph made?
-
Prepare standard tubes. Each has a different, known concentration of sodium pyruvate (or oxaloacetate).
-
Run the full color reaction. Add reagents and let color develop in a set time, just like you would for your test sample.
-
Measure absorbance. Use the colorimeter for all standards and write down the numbers.
-
Plot the points. Put each absorbance value on the graph and match it with the Karmen unit for that tube.
-
Draw the curve. Connect the dots—you'll see how the absorbance changes as the Karmen units go up.
How do you use the graph?
-
Measure the absorbance of your test serum sample.
-
Find that absorbance on the Y-axis of your calibration curve.
-
Move horizontally to see where you hit the curve, then drop down to the X-axis.
-
Read the corresponding Karmen unit. This gives you the enzyme activity for your test sample.
Why do it this way?
-
Sometimes the color response doesn't increase in a straight line (not perfectly linear), so using a graph makes sure you always get the right value for your sample.
-
It corrects for small differences between reagents, equipment, or setup each time you run the test.
Method
-
Use the observed absorbance of test serum to locate corresponding Karmen units from the calibration curve.
-
For example, if Abs530 (SGOT) = 0.11, the graph shows 38 Karmen units; Abs530 (SGPT) = 0.15, the graph shows 105 Karmen units.
-
Normal reference (adults): 20.83–83.33 Karmen units (10–40 U/L)
-
Men may have slightly higher values.
-
Karmen unit/ml ≈ 0.48 U/L
-
RESULTS
-
Plot the calibration curve and mark where your test absorbance falls.
-
Report Karmen units for SGPT and SGOT.
-
Compare with reference range.
CONCLUSION
Elevated values of SGPT (ALT) and SGOT (AST) enzymes reflect liver cell injury. Interpretation based on relative levels and the AST/ALT ratio distinguishes hepatitis, alcoholic liver disease, myocardial infarction, or cholestasis. The colorimetric Reitman & Frankel method offers a rapid, reliable strategy for routine LFTs in clinical labs. Results must be correlated with clinical history and other LFTs for accurate diagnosis.
Precautions:
-
Use fresh serum, avoid hemolysis and contamination.
-
Prepare reagents and calibration standards accurately and freshly.
-
Preserve substrate with a small quantity of chloroform if not used at once; discard on turbidity.
-
Incubate samples precisely for optimum reaction.
-
Interpret enzyme elevations within clinical context.
Summary Table of Interpretation
| SGPT/SGOT Result | Likely Interpretation |
|---|---|
| Normal (<40 U/L) | Healthy liver function |
| Mild increase (40–100 U/L) | Early cell injury, fatty liver |
| Moderate increase | Viral/acute hepatitis, drug toxicity |
| AST > ALT, ratio >2 | Alcoholic hepatitis, cirrhosis, extrahepatic damage |
| ALT > AST, ratio <1 | Acute viral hepatitis, severe hepatocellular damage |
| >1000 U/L | Massive necrosis, severe acute liver injury |
Draw a curve of Karmen units on X axis versus absorbance on Y axis
|
A 530 GOT |
0.11 |
|
A 530 GPT |
0.15 |
